The methods behind our investigation of serious mental illness and abuse citations at nursing homes
by ELISABETH GAWTHROP | August 7, 2025
Like our initial investigation of nursing homes, which was specific to California and led by LAist, our recent national investigation relied on data obtained via a Freedom of Information Act request to the U.S. Centers for Medicare & Medicaid Services (CMS). The data we received, called the “Minimum Data Set” (MDS) covers the years 2013 through 2023. We did not find a significant trend nationally in our data, and so we focused on the latest year in our analysis and story.
The data set includes assessments CMS receives of all residents from all nursing homes eligible to receive funding from Medicare or Medicaid — which constitutes nearly all nursing homes. We used the MDS data to analyze the approximately 15,000 skilled nursing facilities (“nursing homes”) appearing in these records nationwide.
Our analysis included many steps to turn these millions of assessments into a facility-level census and then to calculate measures of serious mental illness by facility, state and for the country, as outlined below. We also incorporated information from other CMS datasets. In addition to this narrative description, please see our GitHub repository for the code used in the analysis, which was conducted in the R programming language.
1. Creating a yearly census of nursing home residents
We identified all people from each year of data whose final assessment was not a discharge, thereby creating a census of people in a skilled nursing facility on Dec. 31 of each year. We then found the latest-dated assessment containing diagnosis data for each of those people.
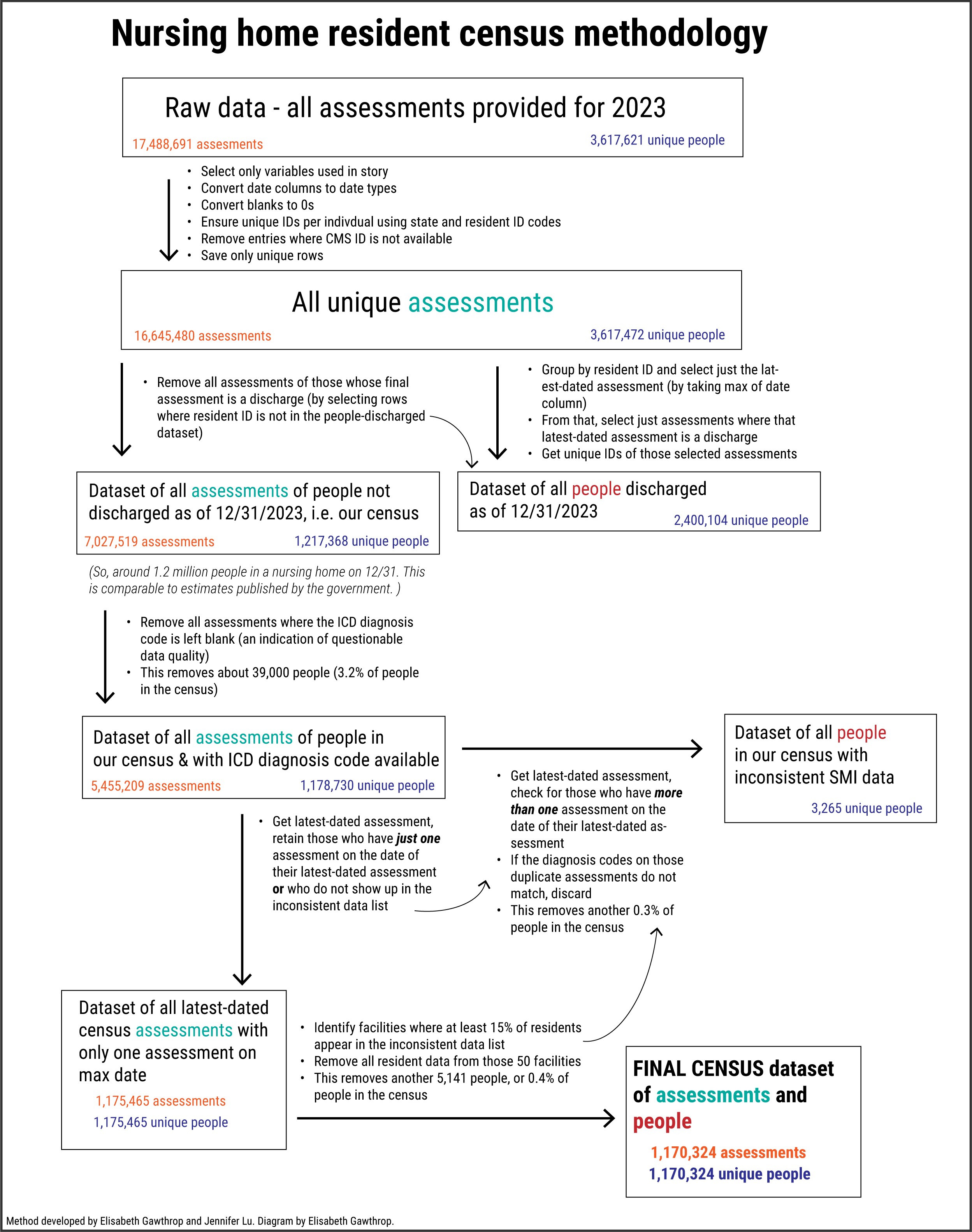
If a resident did not have diagnosis information available, they were excluded from the census. Others were excluded if there were multiple assessments on the same date with conflicting diagnosis data, or if the facility where there were was missing data for at least 15% of its residents. The share of total nursing home residents who were excluded in 2023 was around 4%.
2. Identifying patients with serious mental illness
MDS has specific variables indicating whether a resident has a certain condition, including a range of mental illness diagnoses. We defined serous mental illness as a diagnosis of bipolar disorder, schizophrenia, psychotic disorder or some combination. While depression, anxiety and post-traumatic stress disorder can fall in the category of serious mental illness, we used the "narrow definition" as described in the 2019 PASRR National Report.
(PASRR, the Preadmission Screening and Resident Review, is conducted when people are being considered for admission to nursing homes.)
3. Creating a list of specialized nursing homes, guided by state policy
In addition to information about nursing home residents, CMS publishes datasets with information about nursing home facilities, including staffing levels and whether they are run by a nonprofit, for-profit or governmental entity. These datasets also include information about the number and types of citations issued by the government, if any, received by each facility, as well as fines levied by CMS.
The data set does not include information about whether a facility may have some sort of official allowance to provide care for those with serious mental illness. Some states have policies that officially provide for this type of oversight or allowance. We wanted our summary statistics to only include nursing homes with no oversight, additional reimbursements or government control specifically related to care for mental illness. So, we requested a list of such facilities from oversight bodies, typically health departments, in all states.
In some cases, there wasn’t a clear answer on whether facilities with special oversight for mental illness exist in the state. We erred on the side of excluding any facility that a state mentioned in their communications with us as being on its radar that it cared for people with serious mental illness. There were also a few states from whom we didn’t hear back, but we found evidence of nursing facilities run by the state’s mental health department. Those are also included. The table below provides a summary of what we found.
4. Analysis: Testing for differences
Once we had assembled the comparable list of facilities and nursing home residents within each facility, we were able to conduct a series of analyses, comparing:
Rate of serious mental illness by ownership status (for profit versus nonprofit or government)
Number of abuse citations by rate of serious mental illness
Staffing levels by rate of serious mental illness
Number of abuse citations by ownership status and rate of serious mental illness
Number of abuse citations by ownership status, staffing levels and rate of serious mental illness
Fines issued per abuse citation, and for facilities above and below the 50% serious mental illness threshold
Rates by state
We tested to make sure that serious mental illness rates had an effect on abuse citation rates independent of staffing levels, using linear regression.
‘We did not want to take this guy’:
Abuse rates higher at nursing homes with more mental illness
While we excluded the specialized facilities for most of our analyses, we did take a look at abuse citation rates for these facilities. In most states with at least five such facilities, there were more abuse cases at the facilities with the specialization than without. However, when looking across all states with such facilities, the specialized facilities with high rates of serious mental illness had on average fewer abuse citations than facilities with high rates of serious mental illness that weren’t specialized. On the other hand, specialized facilities with low rates of serious mental illness had on average more abuse citations than facilities with low rates of serious mental illness that weren’t specialized. This is why we report mixed results in the story.
For the specific code used in our analyses, see our GitHub repository.
5. Illinois-specific analyses
We also conducted two analyses specific to Illinois. The first was to use the same methods we used for the 2023 resident census, but for 2013, to compare if and how the rate of serious mental illness had changed in the state over that decade. However, while today Illinois has no nursing homes in the MDS that are designated for mental illness care, it did in 2013. We removed those facilities to be consistent with the rest of our analyses and with the 2023 data.
We also removed resident data where the CMS identification number was not listed. Although there is an internal facility ID number also available in the data, we could not use that to determine if a facility might be one designated for serious mental illness. The removed data — about 1,5000 residents — did have a high rate of people with serious mental illness. So removing that data drove down the 2013 serious mental illness rate by about a percentage point. Had this data been included, and if none of those people were at a specialized facility, the change from 2013 to 2023 would have been 3.3 percentage points instead of 4.5 points.
The second Illinois analysis that we did was examine the primary diagnosis of nursing home residents, by facility. This is a variable in the MDS that’s not available for every state. The primary diagnosis of a resident indicates the International Classification of Diseases (ICD) code that best describes the reason the resident needs skilled nursing care. Medicaid regulations refer to this as a chief indicator when determining whether or not a facility is functioning as a mental health institution. If most residents are there with a primary diagnosis of mental illness (that’s not dementia or Alzheimer's), that facility is arguably serving as a mental health facility.
We followed the same census methodology, this time selecting for the primary diagnosis code availability. We then calculated the percent of residents with a primary diagnosis related to mental illness. We used ICD codes beginning with F2, F3, F4 and F6 to define mental illness. The broad categories associated with these codes are schizophrenia, psychotic disorders, mood disorders, anxiety and personality disorders. (Unlike in the other MDS analyses, we broaden beyond the narrow definition of serious mental illness, under the assumption that if someone’s mental illness is the main reason they need care, it is serious.)